

I’ve been following the various trials and have been interested in the response rates and value of using a four-drug combination (a quadruplet) versus a triplet (a three-drug regimen).
The last few years, we have been learning about the response rates, side-effect management, and real-world evidence of utilizing quadruplets versus triplets. I’m not a fan that adding more drugs is always a good thing, and I come from the early days of just using one drug at a time. However, with the last dozen+ years of following the growth in research in myeloma and the many recent approvals and improved response rates, overall survival, and quality of life, we can better manage multiple drugs to fight the myeloma from a variety of mechanisms of action.
Example: at ASH 2019 we learned from the GRIFFIN study update that the depth of response to Darzalex + Velcade, Revlimid and dex (D-VRd) improves over time in patients with transplant-eligible, newly diagnosed myeloma. Adding Dara to VRd improves response rates and depth of response, including stringent complete response (sCR) and Minimal Residual Disease (MRD) negativity. All great news, right?
My question to a number of myeloma specialists was based on the utilization of Dara. Once patients attain MRD- their doctor may recommend to stop the Dara and only continue with VRd. By doing this, and if you relapse while only on VRd, you may be able to add the Dara back in since you would not be refractory to Dara. This may be able to extend a patients time utilizing this drug combination.
An early phase 1b/2 study I found interesting was:
1011 Sonrotoclax (BGB-11417) in Combination with Dexamethasone for the Treatment of Relapsed/Refractory Multiple Myeloma with t(11;14): Safety, Efficacy, and Determination of Recommended Phase 2 Dose
Hang Quach, MD, FRACP, FRCPA, MBBS
This is similar to venetoclax, a first-generation BCL2 inhibitor that has demonstrated antimyeloma activity as a monotherapy or combination treatment but has no regulatory approvals for mulitiple myeloma.
Sonrotoclax, a next-generation BCL2 inhibitor, has shown more potent and selective BCL2 inhibition and better activity against BCL2 than venetoclax in vitro.
In our support group, we have a member on venetoclax and doing well. However, her concern is that as a patient with translocation (11:14), what’s next? This could be a future option to pay attention to, although a very small, early trial.
Another early phase I trial that is hopeful is the following:
Sumit Madan, MD
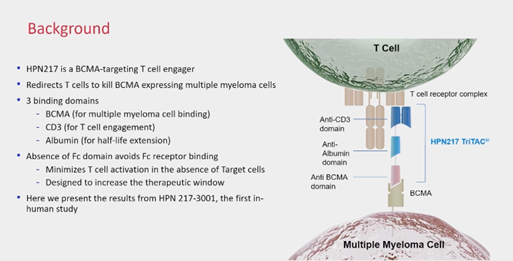
HPN217 is a half-life extended tri-specific T Cell engager. While some tri-specifics in myeloma connect CD-3 to two targets on the myeloma cell, such as BCMA and GPRC5D, the HPN-217 has 3 binding domains: BCMA, CD3, and albumin (for half-life extension).
IMF Chief Medical Officer Dr. Joseph Mikhael explained this to us in our Myeloma Voices working meeting that HPN-217, one arm hooks onto the T Cell CD3, and the other arm hooks on to BCMA (on the myeloma cell) and the third arm hooks on to albumin, which is the most abundant protein in the blood. This helps to work as a time-release type therapy so perhaps fewer infusions would be required.
Again, another early but interesting trial to watch.
Lots of early science here but very promising and I will continue to watch these as they progress. With so many options, the sequencing of CAR-Ts and bi-specifics and tri-specifics will be something our myeloma community will be watching closely.
In closing, I’ll share that I’ve been attending ASH since around 2004 and the Minnesota Vikings always play while I’m at ASH. Every year, they’ve lost! But this year, that changed and the Vikings won 3-0. In my last blog I wrote about Time and how it changes and included a song, so for this blog I’ll continue with the theme of Time and Change plus the Vikings win. Enjoy Minnesota Fans: SKOL!
Fight, Fight, Fight, Fight Myeloma!