
Day 0 Blog 2
The second symposium I attended (in sweatpants and fuzzy slippers) was CAR T-cell therapies in relapsed/refractory multiple myeloma: evaluating the evidence for optimal integration, presented by Drs. Sikander Ailawadhi and Ajai Chari. Learn more here.
I admit I was a little worried that this was going to be so far over my head and that I’d not be able to say anything about it. I was “kinda” wrong; I did understand quite a bit! First of all, it seems to me (and later affirmed) that of the 2 available CAR T treatments, cilta-cel is better in most circumstances than ide-cel.
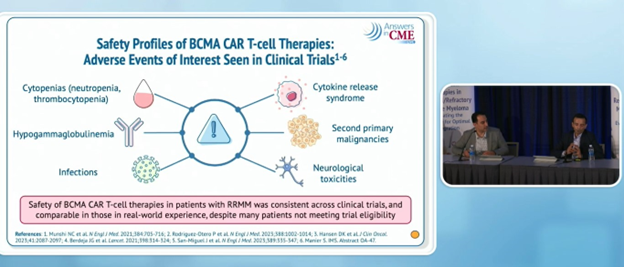
Adverse events are pretty well known, especially cytokine release syndrome (CRS) and neurotoxicity. There’s been a bit in the news lately about second primary malignancies, but these are very rare. In fact, most cancer treatments carry this risk. Sometimes, a defect in the patient’s original T cells can cause a problem. The Bottom Line: In these doctors’ opinions, the benefits far outweigh the risks.
Of the more serious side effects is the Parkinson-like disease that can develop later, which raises the importance of engaging the community physicians in the ongoing care of these patients when they return home, often far from the medical center where they received the CAR T-cell therapy.
Further discussion was about the role of bispecifics. In most instances, they said that it would be preferable to administer CAR T before bispecifics. One of the concerns is that bispecifics cause T-cell exhaustion, making them less able to be manufactured for the treatment.